
History of Drug Addiction and Alcoholism Epidemics in America » Addiction Unscripted
People are dying. We are in the midst of the third drug epidemic in the last 50 years and the second one involving opioids. And although its victims have at least garnered enough attention to push lawmakers towards many radical approaches to drug policy reform, the reaction to the contemporary drug epidemic is very different from the way these epidemics were treated in the past. Perhaps even curiously different.
Today’s crisis is being treated as a public health issue. Given America’s history of dealing with drug epidemics, this kind of reaction is unprecedented. And although it could lead to better prevention and treatment for addiction and a more compassionate view of people with substance use disorders, there is also frustration.
This is precisely because of how at odds it is with what U.S. citizens have come to expect when it comes to drug issues. Overall, it’s a positive change, but it’s a change that should have happened years ago. It’s also unclear whether this contrasting perception of addiction as a public health issue stems from a learned history of what hasn’t worked, the visibility of deaths from overdoses, or the demographic profile of people the current epidemic is largely affecting.
THE OPIOID EPIDEMIC
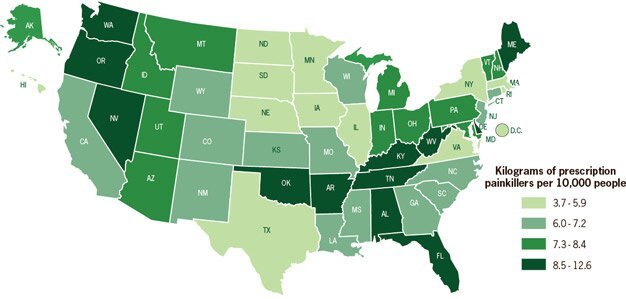
In 2014, for the first time in recorded history, more people died of drug overdoses than car accidents. About half of those deaths were caused by opiates (e.g., oxycontin, heroin), costing approximately 29,000 lives. And although prescription opiate overdoses have been on the rise since the turn of the century, the most recent concern centers on the surge of heroin use and heroin overdoses.
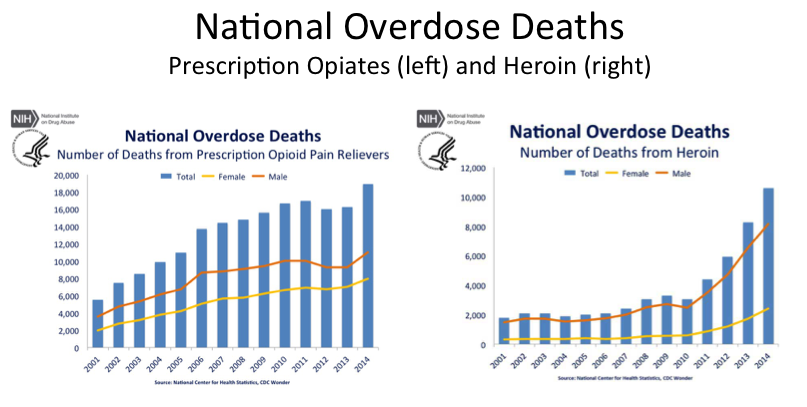 Adapted from NIDA website: http://www.drugabuse.gov/related-topics/trends-statistics/overdose-death-rates
Adapted from NIDA website: http://www.drugabuse.gov/related-topics/trends-statistics/overdose-death-rates
Heroin and prescription opioids share essentially the same mechanism of action. Both act on several types endogenous opioid receptors in the central nervous system, which in turn relieves pain, causes euphoria, and manipulates the reward system. However, the most important difference between the two is purity. Prescription opiates are much more pure than heroin, and by consuming them in unintended ways, such as crushing then smoking, snorting, or injecting them, the euphoria is much more immediate and intense. Thus, the addiction liability is high.
Even though prescription opiates are “better” drugs, several factors have contributed to the increase in heroin abuse in the last five years and subsequent spike in heroin overdoses. Doctors became more cautious in the face of increasing prescription opioid overdoses; drug companies developed new pill types (e.g., extended release) to counter opioid abuse; and legislation introduced new pain clinic laws. These regulatory factors limited access to legal opiates for everyone. Subsequently, individuals with substance use disorders started buying heroin on the black market, where prices had dramatically decreased by about 80% since the 90’s, while at the same time the relative purity of heroin had increased by about 60%.
It’s true that the resurgence of heroin in the U.S. is a problem, but it’s the reaction that has piqued my interest. It seems as if no one is suggesting we should lock up the people who are caught in the middle of this epidemic, nor is anyone demanding stricter laws and harsher punishments, or suggesting residents hide their children from crazy “junkies” and gun-toting gangsters. In fact, what people are saying is that individuals with opiate-use disorders need help. It’s exactly what those of us in the addiction field have come to expect: a sympathetic reaction to a debilitating disorder. But, the reaction by everyone from law enforcement to journalists to politicians is more than a little baffling.
To understand why, consider the previous drug epidemic and its consequences.
THE CRACK EPIDEMIC
Before the 1980’s, cocaine use was confined to a select number people and an even smaller number of people smoked it (aka freebase cocaine). But around 1983, crack exploded in the inner cities of San Francisco, Philadelphia, New York, and other large cities, primarily affecting disadvantaged areas. Once it reached a threshold, capturing the attention of the media, the hype spun out of control, and it was soon deemed a crack epidemic. In hindsight, it was likely more of a crack scare that precipitated the epidemic. At the time, however, it was viewed as drug pandemonium, and the consequences of the crack epidemic were drastic and unfortunate.
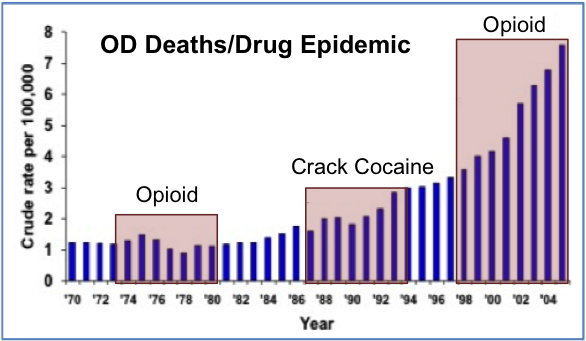 Adapted from http://www.pdmpexcellence.org/content/overdose-deaths – The source: National Vital Statistics System
Adapted from http://www.pdmpexcellence.org/content/overdose-deaths – The source: National Vital Statistics System
Unlike the current opioid epidemic – which has captured our attention due to the number of overdoses – deaths directly associated with crack ingestion were minimal. Overdose deaths associated with crack did increase from the early 80’s to the early 90’s, but the numbers pale in comparison to opioid overdoses today. It was the indirect effects of crack that proved to be so devastating.
Shortly after crack cocaine was introduced into the U.S., politicians started enacting strict laws to try and curb the violence that was related to the crack trade. In 1986, Congress passed the Anti-Drug Abuse Act, which created mandatory minimums for crimes associated with drug dealing. Crack was singled out as the most dangerous, more so than cocaine, even though they are the same drug. A harsh 100 to 1 crack to powder cocaine disparity was enacted. Only five grams of crack, compared to 500 grams of cocaine, triggered a five-year mandatory minimum, and 50 grams of crack vs. five kilograms of powder cocaine triggered a 10-year mandatory minimum.
That was for first-time offenders. What about the second offense? That doubled the penalty. And, third? Life.
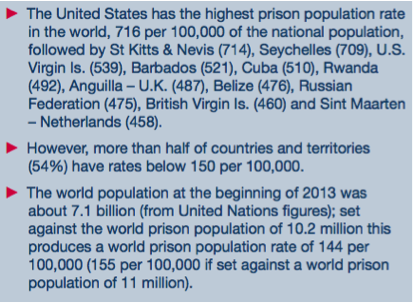 International Centre for Prison Studies
International Centre for Prison Studies
In 1988, the 100 to one crack to powder cocaine disparity was applied to simple possession, not just dealers and traffickers. It could be argued that policies like mandatory minimums started a snowball effect wherein the newly increased amount of imprisoned non-violent drug offenders eventually led to over an eight-fold increase of inmates in the federal system and the highest overall prison population rate in the world.
Only recently have these severe and damaging laws been attenuated, though not eliminated, creating an 18 to one crack to powder disparity. This is progress, but given the information we have about crack and powder cocaine, a crack to powder cocaine disparity shouldn’t exist. Plus, the recent decrease in disparity should have been applied retroactively, which it wasn’t.
In hindsight, it looked more like a war on the impoverished rather than a war on drugs, based on misinformation that crack was special somehow. These myths have been debunked. It turns out that crack was special, but only from a marketability standpoint. Rocks could be sold for $5-10 a piece on street corners. It’s also smoked rather than snorted, so the high is intense but short lived, lending itself to binge-type use. It’s important to note that theoretically, crack is no more addictive than cocaine. However, both can manipulate the reward system quite well and thus, the addiction potential of both crack and powder cocaine is high.
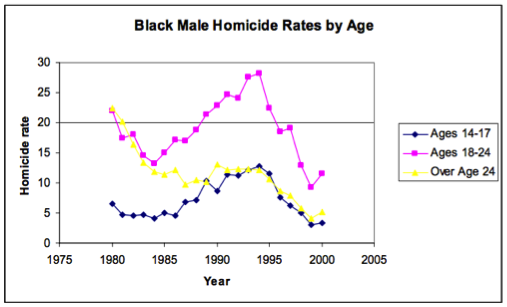
In inner-city communities, especially those suffering economically, crack was seen as a way to move up the financial ladder. It was found to be a lucrative market that drew the interest of street gangs who, up until that time, had little to do with the drug trade. Crack changed all that. As a result, turf wars ensued. In one study, researchers found that, in addition to dramatically increased homicides, the crack epidemic was found to be associated with several detrimental social factors in the black community.
 Fryer Jr. et al., 2005: MEASURING THE IMPACT OF CRACK COCAINE
Fryer Jr. et al., 2005: MEASURING THE IMPACT OF CRACK COCAINE
“We find that the rise in crack from 1984-1989 is associated with a doubling of homicide victimizations of Black males aged 14-17, a 30 percent increase for Black males aged 18-24, and a 10 percent increase for Black males aged 25 and over, and thus accounts for much of the observed variation in homicide rates over this time period. The rise in crack can explain 20-100 percent of the observed increases in Black low birth weight babies, fetal death, child mortality, and unwed births in large cities between 1984 and 1989. In contrast, the measured impact of crack on Whites is small and statistically insignificant.”
So even though the crack epidemic was not responsible for as many overdoses as the current opioid epidemic, the prohibition of cocaine and the sales potential of crack created a ripe opportunity in low-income communities for dealers and gangs, already accustomed to high-risk living, to make fast cash and resort to violence in settling disputes. The consequence was significantly increased homicides, particularly in adolescents. Plus, strict new drug laws plucked inner-city residents from their homes and communities and sent them to jail for many years, making it even more difficult for the families left behind. This also made it hard to integrate back into society following a felony drug charge. Taken together with actual drug overdoses, it’s likely that the crack epidemic cost as many lives if not more than what society is witnessing today with the opioid epidemic.
what we’ve learned
So what do we make of all of this? Hopefully, we’ve learned from history and are genuinely trying to approach the drug epidemic from a more realistic perspective.
But perhaps it’s the class and color of the addiction sufferer that mattered and still matters today. If history is to repeat itself and there is a shift from primarily white users to black users (as was evident in the first opioid epidemic in the 1970’s), severe punishments may return for opioid users. Maybe the victims of the current opioid epidemic existing everywhere in America elicit our compassion, and we think we understand the underlying corruption that caused these premature deaths. Someone or something caused these deaths, and their potential as a productive member of society is obvious. Indeed, something must be done to help them.
But, in the inner city, we hear little from the families. No amplification of their voices as they mourn in silence for yet another casualty. One that’s far too common and so easy to ignore. There’s a separation between inner-city residents and law enforcement, not to mention government officials. We perceive chaos surrounding the victims, and a brutality leading to their demise.
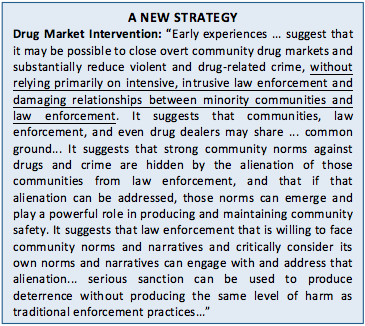 The High Point Drug Market Intervention Strategy
The High Point Drug Market Intervention Strategy
Very few wanted to examine the tragedy of the crack epidemic, the fact that families were economically deprived, and that crack was seen as an opportunity to escape the hardship of disadvantaged living. Fortunately though, some did. Consequently, new programs like the Drug Market Intervention are being tried that attempt to reinvigorate communities with drug markets by bringing together law enforcement, community members, and community leaders. Encouragingly, the results so far have been very positive.
It’s still unclear whether we’ve learned from the past, and only time will tell. But this new type of strategy, along with the way society is reacting to the current drug epidemic, suggests that we may actually be ready to move forward and approach the drug problem differently: more empathetically, more intelligently, and with an eye on historical missteps. Or at least one can hope. People suffering from addiction as well as people in less fortunate circumstances deserve that level of attention, as well as our hearts and minds, so that we can find creative solutions to this critical issue and provide help, not punishment.