

The Science Behind Why Psilocybin Could Be The Next Cannabis » Addiction Unscripted
Given the mounting evidence for their medical benefits, magic mushrooms could be the next substance to challenge the legal status quo. But can they succeed? Here’s why we should legalize ‘shrooms, and why we won’t.
After “Sandra” was diagnosed with advanced ovarian cancer, she underwent the conventional treatments: her tumor was excised and she withstood an exhausting months-long regimen of chemotherapy. But even as her physical symptoms went into remission, Sandra’s anxiety did not. Her emotional eating grew out of control. Each oncology appointment was fraught with terror that her cancer could return. Nothing seemed to help. Nothing, that is, until Sandra tried psilocybin, reported Jennifer Bleyer in her excellent original coverage of Sandra’s story in NYU Alumni Magazine.
Sandra received her psilocybin treatment in a safe, supervised setting as part of a research study at NYU’s Cancer Institute. Lying on a comfortable couch in a silent room, she donned eyeshades and headphones. Soon the hallucinogenic trip came on, and Sandra saw her own body from without, consumed by a black mass. This was a manifestation of her own fear threatening to eat her alive. But Sandra resisted, the blackness faded, and she felt enveloped in a profound glow. As Sandra later recalled to Bleyer: “I was… [t]otally bathed in love. It wasn’t just my love for my children and my husband and my dearest friends — it was their love for me. It was all part of the same thing. I felt timelessness, that I was part of an eternal existence. It was the most magical, wonderful experience I’ve ever had in my life.”
Pause here, and we’d have just another trippy drug story. But the magnificent part of Sandra’s case is not her trip, but what happened after her trip was over. Sandra’s sense of calm stuck with her long after the treatment. Months passed, and she continued to feel grounded; she stopped overeating; she made new friends. Her fear of cancer had disappeared.
Sandra’s anecdote is not an anomaly, nor is she the only intrepid adventurer who’s boldly stepped forward to get totally stoned in the name of science. Researchers at myriad institutions have independently corroborated psilocybin’s efficacy in alleviating mood disorders. Dr. Charles Grob at Harbor-UCLA Medical Center studied anxiety in advanced-stage cancer patients and reported significant reductions in anxiety and/or depression at intervals of 1, 3 and 6 months. Stephen Ross, the head of the research team who treated Sandra at NYU, had undertaken similar work with equally promising results. As Ross told Aeon magazine: “Patients would tell me that they’ll never be able to get out from under the rock that hangs over them… with the fact they have cancer. But those feelings evaporated under the influence of psilocybin. They almost uniformly experienced a dramatic reduction in existential anxiety and depression, and an increased acceptance of the cancer, and the changes lasted a year or more and in some cases were permanent.”
While the psychic burden of a cancer diagnosis makes these patients a particularly vulnerable population, the boon that psychedelics provides does not appear to be limited to acute, situational mood disturbances. In Journal of Psychopharmacology, Dr. Peter Hendricks, et al., reported that lifetime use of classic psychedelics (including psilocybin) correlated with significantly reduced odds of psychological distress, suicidal ideation, and suicide attempts, whereas lifetime use of other illicit drugs is generally associated with increased likelihood of such negative outcomes. Hendricks concluded that “classic psychedelics may hold promise in the prevention of suicide, supporting the view that classic psychedelics’ most highly restricted legal status should be reconsidered to facilitate scientific study.”
At Johns Hopkins School of Medicine, Roland Griffiths, et al., found that administering psilocybin to hallucinogen-naïve subjects induced positive mystical experiences and “…sustained positive changes in attitudes.” Significantly, mental wellbeing was not confined to patients’ self-perception; Fourteen months after the experiment, friends, family members, and colleagues independently confirmed that test subjects had grown calmer, happier, and kinder since their use of psilocybin.
Further studies have produced promising results suggesting psilocybin could play a role in treating obsessive-compulsive disorder, alcohol and tobacco addictions, cluster headaches, and as an adjunct to psychotherapy that would facilitate patients’ recall of salient positive memories and reverse innate negative cognitive biases.
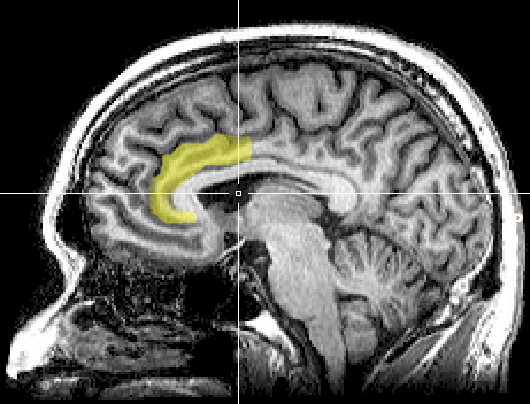
So how does psilocybin work this magic? Researchers at Imperial College London used functional magnetic resonance imaging (fMRI) to study the brains of test subjects while tripping and observed diminished activity in the anterior cingulate cortex, a region known to be overactive in individuals with depression. Similarly, the fMRI revealed hemodynamic effects in the default mode network, a neural system activated when the individual engages in inward-focused tasks such as memory retrieval or daydreaming of the future. Essentially, psilocybin acts as “off switch” for the affected neural circuitry. As researcher David Nutt told The Guardian, “People with depression have overactive default mode networks and so ruminate on themselves, on their inadequacies, on their badness, that they are worthless, that they have failed… psilocybin appears to block that activity and stops this obsessive rumination.” Nutt further emphasized the need for novel treatments for depression, noting that only a third of depressed individuals respond fully to conventional treatment with antidepressants, and 10% fail to respond entirely. “We badly need more types of treatment but we cannot pursue these because the government is denying scientists access to powerful tools that could help people in need. The regulations that govern researchers access to Class A drugs are totally inappropriate and harmful.”
Herein less the catch-22 for a scheduled substance seeking to prove its medical pedigree. Research on restrictively scheduled drugs is difficult to fund because they are considered dangerous and not useful. Simultaneously, restricted drugs are considered dangerous and not useful due to a lack of concrete research results to show otherwise. In the USA, psilocybin is a Schedule I Controlled Substance, a legal category defined by criteria including: (1) a high potential for abuse; (2) no currently accepted medical applications; and (3) a lack of safety in use. Schedule I is reserved for the “worst” drugs, while throughout Schedules II through V, each progressive category contains drugs that are “lesser” than the previous. For comparison, Schedule I contains heroin, marijuana, ecstasy, and magic mushrooms; Schedule II contains cocaine, crystal meth, and oxycodone; Schedule III contains anabolic steroids and barbiturates; and so on. The placement of magic mushrooms in a category worse than meth reflects the tarnished history of the drug — widespread use of psychedelics in the 1960s and 70s scared the establishment into cracking down on Timothy Leary’s cronies, for fear that an entire generation would “turn on, tune in, drop out.”
Now that the hysteria is a few decades behind us, a more discerning examination of the evidence reveals that magic mushrooms do not meet the defining criteria for a Schedule I drug: they do not have a high potential for abuse; they have useful medical applications; they are generally regarded as safe, when used responsibly. Although our primary focus is medical efficacy, let’s examine briefly the safety and abuse potential.
In a double-blind, placebo-controlled study, Hasler, et al., administered varying dosages of psilocybin and monitored blood pressure, heart rate, cortisol levels, and other physiological measures of bodily stress. His team found “no cause for concern that [psilocybin] is hazardous with respect to somatic health.” Johansen, et al., used a population study to look for correlations between psilocybin and health problems at a broader societal level: “We failed to find evidence that psychedelic use is an independent risk factor for mental health problems. Psychedelics are not known to harm the brain or other body organs or to cause addiction or compulsive use; serious adverse events involving psychedelics are extremely rare. Overall, it is difficult to see how prohibition of psychedelics can be justified as a public health measure.”
In The Lancet, the UK’s Independent Scientific Committee on Drugs used a multifaceted analysis to rank prevalent drugs in terms of their harm-causing potential, as categorized by 16 variables within the larger sub-categories of damage to the self (e.g. dependence, loss of social relationships, cognitive impairment, etc.) and damage to others (e.g. crime, environmental damage, family adversities, etc.). Magic Mushrooms were the least harmful of all studied drugs.
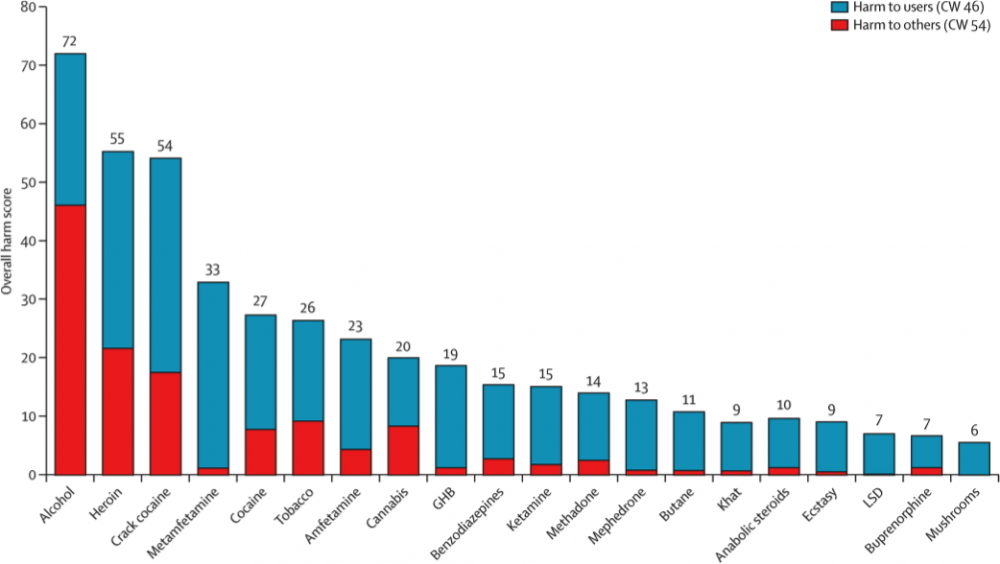
Data courtesy of Independent Scientific Committee on Drugs
This is not to say that mushrooms are universally harmless. Licit or illicit, all drugs have potential to cause harm. Mushrooms should emphatically not be used to haphazardly self-medicate, particularly by those who might be at risk for schizophrenia or other forms of psychosis. Nor should they be used by minors, whose brains are still developing. I don’t propose that ’shrooms be legalized entirely, rather, that they be treated like other psychoactive prescription drugs on Schedules II or III, such as codeine or valium; we should restrict their use to patients who can take them safely, under the supervised eye of professionals, and who stand to benefit from their effects.
To the extent that mushrooms do present risks, the dangers generally involve the panic a user experiences while on a “bad trip.” Psychedelics can elicit temporary feelings of terror and confusion, but lasting effects are quite rare. Historically, there has never been a recorded overdose of psilocybin.
Because mushrooms greatly impair the senses if taken in high doses, it could be wildly dangerous for users to undertake activities that require coordination and judgment while tripping — as with alcohol, it could be fatal to get behind the wheel of a car, to go rock climbing, to operate a chainsaw, etc. Of course, this risk already exists with current users of psychedelics, but could become more widespread if use proliferates. That said, medical mushrooms might mitigate this danger by offering a controlled setting for use, as was done in for Sandra at NYU.
As for abuse potential, mushrooms users do not appear to struggle with addiction. While some people are regular users, temporary tolerance discourages overly-frequent tripping: a dose that produced strong effects on one day will have little effect if taken the next day. Over time, the tolerance decreases until the user is again sensitive to the drug. Moreover, the research suggests that only a few medicinal doses are required to effect lasting changes — not necessarily regular lifelong use — and medical professionals could schedule these doses at intervals most appropriate to patient care.
While an objective look at the risks and benefits of psilocybin clearly indicates it would be more properly placed on a lower federal schedule, its re-scheduling is not likely any time soon, due to lack of sufficient political cache. There’s not exactly a groundswell of peasants rising up with pitchforks and torches to encircle local legislative offices demanding access to ‘shrooms. (Although one group of sponsors in Washington State have undertaken a legalization initiative modeled on Initiative 502, the state’s marijuana reform.)
But federal re-scheduling is not necessarily prerequisite to wider use and acceptance. Consider the parallel case of marijuana: at this moment in history, the sea change in marijuana’s legality remains incomplete but feels increasingly inevitable. Currently, 23 states allow medical marijuana use, 17 have taken measures of decriminalization, and pot is wholly legal in four. Water cooler speculations over which states will be next cite those traditionally at the fore of social progress — think California and Massachusetts — but also those such as Arizona or Missouri, where the arguments gaining political traction tend to be more Ayn Rand than Willie Nelson. But despite this state-by-state proliferation, so-called “medical” marijuana remains federally a Schedule I Controlled Substance.
The American Medical Association has urged that cannabis be re-scheduled to a less restrictive class to enable future scientific scrutiny, while simultaneously recommending that marijuana should not currently be used medically due to lack of proven efficacy. The AMA is absolutely right. Despite the increasing public perception that marijuana is legitimate medicine, evidence for the effectiveness of medical marijuana is actually less overwhelming than you might think. The Journal of the American Medical Association recently published a comprehensive review of all the best available literature, in which researchers found: “moderate-quality evidence to support the use of cannabinoids for the treatment of chronic pain and spasticity [and] low-quality evidence suggesting that cannabinoids were associated with improvements in nausea and vomiting due to chemotherapy, weight gain in HIV infection, sleep disorders, and Tourette syndrome”; however, none of these positive associations were of statistical significance. As for other commonly accepted conditions purported to be treated by medical cannabis — such as glaucoma, diabetes, Crohn’s, IBS, and dementia — scientific evidence of the drug’s efficacy is lacking.
Doctors have argued that so-called “medical marijuana” is a front for recreational users, and the great majority of medical cardholders are probably misusing the laws just to get high. Consider that statistically the most common medical marijuana user is a male under 30 who first started smoking pot in his teens, and that seventy-five percent of medical marijuana patients list “pain” as their only symptom. While I don’t discount the importance of pain relief nor the immense degree of suffering experienced by those in irretractable chronic pain, pain alone is nonetheless subjective and easily faked.
Consider, too, the logical inconsistencies in the medical marijuana legalization process. If we truly thought marijuana was a drug like other drugs, why wouldn’t we simply subject it to the routine processes we have in place for bringing pharmaceuticals to market? The FDA has well-defined testing protocols that a new chemical must pass before it can be sold to consumers. Why is a new SSRI subject to these tests, but we leave it to elected representatives and the judicial system to decide whether or not marijuana is medicine? We wouldn’t vote on whether Prozac is medicine. The notion is ludicrous.
As marijuana’s acceptance grows, we grow more comfortable admitting that the “medical” label is a facade. As the first state to legalize weed for recreational use, Colorado was not only a legislative harbinger but also a rhetorical game-changer. No longer were pot advocates restricted to talking about dreary senescent conditions like glaucoma and diabetes; citizens came out in droves to cast ballots for, “Hey, we just want to get high, alright?” Similarly, when Oregon legalized weed, the local rhetoric seemed to have moved beyond “medical.” Oregon’s pro-legalization campaign, Yes on 91, released a statement lauding legalization by emphasizing informed choice: “Oregonians had the wisdom to consider this measure based upon its merits and to move past the outdated information of a failed prohibitionist system.”
For a few specific patients, cannabis may indeed be therapeutic. But for most users, pot isn’t legitimate medicine and thus the medical marijuana movement as a whole isn’t really about medicine; it’s about getting high. But this hasn’t harmed legalization efforts. Because we’re still ostensibly a democracy responsive to the needs of its citizenry (i.e. despite Citizens United), if what the public wants and accepts is decriminalized cannabis, we have the legal framework to advocate for those changes in law.
Herein lies the challenge for mushrooms. While the populace as a whole has grown increasingly comfortable with cannabis, psychedelics are generally perceived as terrifying and threatening in their psyche-altering potential. Despite scientific evidence to the contrary, we still believe it’s common to have a bad trip, fry your brain, suffer a psychotic break, and/or be haunted by trippy flashbacks for the rest of your life. If we made science-based decisions, alcohol and tobacco would be illegal, and your psychiatrist could prescribe ketamine or ’shrooms. Simply put, medical mushrooms probably make too much rational sense for a world still clinging to failed forty-year-old policies to “Just Say No” and lead a “War on Drugs.” As a society, we’re not interested in deciding based on data; we prefer to decide with our hearts and guts. The problem is, our hearts and guts are often wrong, despite our best intentions.
This is why the pro-marijuana movement has succeeded: it’s been enabled by the fact that public perceptions of pot place it more or less on par with beer in terms of intoxication and health risks — although pot advocates will gladly corner you at a party to deliver fervent bullet points enumerating why their favorite herb is in fact less damaging than alcohol, and how this fact implicates inconsistencies in prohibitionary laws. (To this end they can make a halfway decent case only if they aren’t too stoned.) By comparison, mushrooms do not have the same groundswell of popular opinion that would be required for a legalization initiative to gain traction. Maybe attitudes will change in time, as they did for pot. But right now it doesn’t seem likely. Therefore, for medical psilocybin might require a different path toward legality than medical marijuana.
While pot has so far used the shortcut of democratic popular opinion to cheat its way past medical protocol, mushrooms could conceivably prove their worth within the system by passing the same series of clinical trials required for other drugs, as when a pharmaceutical company develops a new statin or antidepressant. Namely, Phase 1 studies must prove safety, tolerability, and acceptable dosage; Phase 2 studies must demonstrate efficacy for treating a medical condition (i.e. anxiety in cancer patients); Phase 3 studies use larger sample size and randomized controls in different locations to verify reproducible treatment value in clinical practice. There are significant hurdles to this pathway, including years-long testing timelines and multi-million-dollar budgets. This immense cost is complicated by the fact that pharmaceutical companies won’t want to pony up investment cash to sponsor such studies, because psilocybin itself is not patentable and because it can make lasting changes in only a few doses, which is the exact opposite of the chemical cash cow a Pfizer or Novartis looks for — what they want is a proprietary drug in a price range that forces users to take out a second mortgage and must be swallowed regularly for life. Perhaps governments, academia, and private citizens will be interested enough to fund mushroom trials efforts, perhaps not. Time will tell.
Considered in the overall framework of science and medical potential, there’s probably already an equal if not stronger case for medical mushrooms than marijuana has ever had. But this conversation is not really about science or medicine. It’s about what we as a people collectively desire and allow, and what we collectively decide to believe in. And until we decide to believe in science, medical mushrooms don’t have a chance.